急診短講013 ─ ARB* Dosage Equivalent
關於 ARBs 劑量的高低,跟降壓效果的強弱,在不同藥物間,不能等同等效。
相同藥物,高劑量 = 高降壓效果。
Potency 如下表:
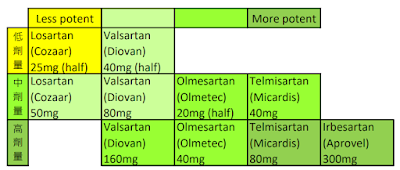
*Angiotensin Receptor Blockers, ARBs

...

急診短講013 ─ ARB* Dosage Equivalent
關於 ARBs 劑量的高低,跟降壓效果的強弱,在不同藥物間,不能等同等效。
相同藥物,高劑量 = 高降壓效果。
Potency 如下表:
*Angiotensin Receptor Blockers, ARBs
...
急診短講012 ─ 關於High dose PPI
針對非靜脈曲張的上消化道出血,常聽到要使用高劑量的PPI,至於高到多少,來看一下證據吧!
【先講結論:針對尚未執行上消化道鏡之前,有大量上消化道出血的病人,給予80mg PPI是個合理的選擇。做完上消化道鏡之後,針對非靜脈曲張的上消化道出血,給予PPI infusion (8 mg/hr for 3 days) 和 intermittent PPI (40 mg twice daily) 之間,沒有很大的差異。運用之妙,存乎一心。】
本文僅針對高風險的出血性潰瘍,包括 active bleeding (I), nonbleeding visible vessels (IIa, NBVV), and adherent clots (IIb) [ () 內為 forrest classification]
也就是P = high-risk bleeding ulcers (active bleeding, nonbleeding visible vessels, and adherent clots)
主要引用Review: An update on the management of non-variceal upper gastrointestinal bleeding. [Gastroenterol Rep (Oxf). 2023 Mar 20:11:goad011.]
ACG guidelines [Am J Gastroenterol 2021;116:899–917.]
Based on 7 RCTs and high-quality evidence
I= high-dose PPI (defined as ≥80 mg daily for 3 days)
C= placebo or no treatment (沒有使用PPI或其他治療,這..沒有武德)
O= further bleeding (RR 0.43, 95% CI 0.33–0.56),
mortality (RR 0.41, 95% CI 0.22–0.79), surgery (0.42, 95% CI 0.25–0.71)
跟不治寮組比較,高劑量PPI顯然有壓倒性好處!
[JAMA Intern Med. 2014 Nov;174(11):1755-62.]
meta-analysis of 13 RCTs
I= Intermittent PPI therapy (40mg twice daily)
C= PPI infusion (80 mg bolus followed by 8 mg/hour infusion for 3 days)
O: all comparable
rebleeding within 7 days, RR 0.74 (0.52-1.06)
need for urgent intervention, mortality, RBC transfusion, length of hospital stay.
跟高劑量PPI組比較,間歇性PPI組治療,有可匹配的效果!
[Aliment Pharmacol Ther 2013;38:721–8.]
meta-analysis of 13 RCTs comparing these two PPI regimens in patients with confirmed high-risk bleeding ulcers.
I= Intermittent PPI therapy (40mg twice daily)
non-inferior to
C= PPI infusion (80 mg bolus followed by 8 mg/hour infusion for 3 days)
O: rebleeding, mortality, and urgent interventions.
間歇性PPI組治療效果,不劣於高劑量PPI組
…
急診短講011 ─ 關於Na的一些事
Sub1: 低血鈉矯正用
定義:
Hyponatremia: Na < 135 mEq/L
Severe Hypo-Na: < 120 mEq/L
輸液選擇:
3% saline 100mL, Na 濃度 513
mEq/L, 100mL總量 51 mEq.
0.9% saline 500mL, Na 濃度 154
mEq/L, 一瓶500mL總量 77 mEq.
(稱不上 "normal" saline
!)
0.45% saline 500mL, Na 濃度 77
mEq/L, 一瓶500mL總量 38 mEq.
非急性低血鈉,矯正速度應低於 8-10 mEq/L/day.
(不適用於急性低血鈉病人 或 SIADH病因者)
根據病人體液狀態、進食能力,選擇合適的 點滴濃度 及 輸液量。
定時追蹤(q4至q8h),再調整。
Sub2: 橫紋肌溶解症治療用
定義:
Rhabdomyolysis: CPK > 5 times the upper
limit of normal OR > 1,000U/L
Severe Rhabdomyolysis: CPK > 5,000U/L
治療目標:
Correction of volume depletion if present (本次主題僅討論輸液調配!)
Prevention of intratubular cast formation
(Volume overload 病人,可併用 利尿劑)
輸液選擇:
0.9% saline 500mL, Na 濃度 154
mEq/L, 一瓶500mL總量 77 mEq.
0.45% saline 500mL, Na 濃度 77
mEq/L, 一瓶500mL總量 38 mEq.
維持足夠排尿,0.5-3 mL/kg/hr
(50-300/hr),高齡者需保守一點。
Severe Rhabdo 可加 Sodium
Bicarbonate
7% 20mL NaHCO3, 1 Ampoule 納含量
16.67 mEq (3 Ampoules = 50 mEq)
1. 需留意沒有以下情況,才可用 NaHCO3.
a. Hypocalcemia is not present,
b. Arterial pH is less than 7.5,
c. Serum bicarbonate is less than 30 mEq/L.
2. 因含 Na, 慎選基本輸液類型, 以避免高血鈉。
若以 0.45% Saline 500 mL 為基底,每瓶加 2 ampoule NaHCO3
前者 Na 濃度 77 mEq/L, 後者濃度 66.7 mEq/L (2 Amp Na量 = 16.7*2 = 33.4 mEq / 0.5L = 66.7)
合計 143.7 mEq/L.
小結論,以 (0.45% saline
+ 2 Amp NaHCO3) 500mL 為一單位,給到足夠的輸液量。
...
實證短講 搜尋策略
PubMed 自 2020 年起更換新介面,
關於搜尋多字字串的透明度(但複雜度)更高,
讓使用者不用費心使用同義字、單複數、英/美式詞彙的轉換,都自動處理好了,
我們只要用 advanced search 的 detail 功能確定一下,了解其背後邏輯即可。
搜尋舉例:
urinary tract infection
PubMed 背後的(自動轉換)搜尋邏輯:
"urinary tract infections"[MeSH Terms] OR
【上段說明:MeSH term】
("urinary"[All Fields] AND "tract"[All Fields] AND "infections"[All Fields]) OR
【上段說明:複數/一般搜尋】
"urinary tract infections"[All Fields] OR
【上段說明:複數/" "精確搜尋】
("urinary"[All Fields] AND "tract"[All Fields] AND "infection"[All Fields]) OR
【上段說明:原搜尋字/一般搜尋】
"urinary tract infection"[All Fields]
【上段說明:原搜尋字/" "精確搜尋】
心得:使用直覺的搜尋字串即可,
1. 除非原搜尋字原型為複數,否則不用刻意用複數搜尋。
2. 在使用其他資料庫搜尋時,不確定有無提供此功能時,
倒是可以參考此模式,以增加搜尋完整度!
3. 若要發表文獻,可以將完整的搜尋語法,寫入內文或附註文件中。
備註:
1. Advanced search details (直接看)

2. Advanced search
download (存檔)
