
顱內出血病患需預防性使用抗癲癇藥嗎?
臨床情境:
57歲男性,因頭痛合併左側肢體無力至急診求診。頭部電腦斷層顯示右側丘腦(thalamus)出血,估計出血量4mL。會診神經外科後,建議控制血壓,及使用預防性抗癲癇藥物。你的疑問:腦內出血病患都需要使用預防性抗癲癇藥物嗎?
(血壓控制請參考:急性中風血壓控制)
聚焦的臨床問題:
P: intracerebral hemorrhage OR intracranial hemorrhage
I: anti-epileptic drugs, levetiracetam (keppra, 神經外科醫師建議用藥)
C: placebo control
O: mortality, convulsion rate, adverse effect
D: systematic review, randomized controlled trials
Q: therapy/prevention type
使用資料庫:
UpToDate, National Guideline Clearinghouse, Medline (PubMed)
UpToDate:
Search terms: adult intracerebral hemorrhage
挑選條目:Spontaneous intracerebral hemorrhage: Prognosis and treatment
Last updated 六月27, 2012
Seizure prophylaxis and treatment:
... If a seizure occurs, appropriate intravenous antiepileptic drug (AED) treatment should be administered to prevent recurrent seizures. (發生癲癇,當然需要使用抗癲癇用藥,和我的病人情況不一樣)
... While some experts suggest a brief period of AED prophylaxis soon after ICH onset as a potential means of reducing the risk for early seizures in patients with lobar hemorrhages. (2007 AHA/ASA指引:專家意見指出,大葉腦出血病患,使用抗癲癇藥物,為降低早期癲癇風險的可行方式)
... 2010 guidelines recommend against prophylactic use of AEDs. (2010 AHA/ASA指引:不建議預防性使用抗癲癇藥物)
哇哇...那到底需不需要用AED(抗癲癇藥物)?
既然UpToDate引用的兩個指引意見相左,所以就來找找原始Guideline到底怎麼寫...
Google搜尋National Guideline Clearinghouse
Search term: intracerebral hemorrhage
挑選條目:(第一條)
Guidelines for the management of spontaneous intracerebral hemorrhage in adults. 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. 2007 Jun. NGC:005680
在Recommendations for Initial Medical Therapy段落
Class I
2. Appropriate antiepileptic therapy should always be used for treatment of clinical seizures in patients with ICH (Class I, Level of Evidence B).
發生癲癇,需要使用抗癲癇用藥,建議等級Class I,證據等級B,意思是:證據等級中等 (來自單篇隨機或非隨機對照研究的結果),治療效果一致且顯著。
Class II
5. A brief period of prophylactic antiepileptic therapy soon after ICH onset may reduce the risk of early seizures in patients with lobar hemorrhage (Class IIb, Level of Evidence C).
腦內出血時,短期間使用預防性抗癲癇藥物也許可以降低早期癲癇的發作,建議等級Class IIb,證據等級C,意思是:證據等級低 (來自專家意見的結果),治療效果較不一致或不顯著。
在guideline最後的NGC Status說明此guideline歷經Mar 2008, Dec 2008, May 2009, July 2010的更新。其中抗癲癇治療在2010有更新。
加上建議等級及證據等級之後,似乎明瞭不少!
使用PubMed搜尋一下吧。
前面資料庫及guideline所使用的最新文獻只到2010年,所以使用PubMed的重點,就是2010以後的高品質文獻!
搜尋結果如下,
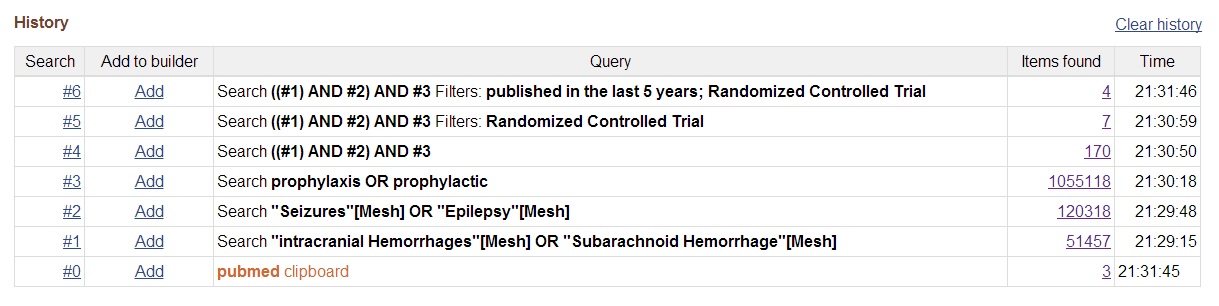
找到主題相符的三篇文章,結果如下,

小評讀一下:
#1. Are post intracerebral hemorrhage seizures prevented by anti-epileptic treatment? Epilepsy Res. 2011 Aug;95(3):227-31. PMID: 21632213.
P: non-traumatic, non-aneurysmatic spontaneous intracerebral hemorrhage (SICH) 自發性腦出血
I/C: valproic acid (VPA) or placebo (Pbo) immediately after a SICH for 1 month
O: occurrence of seizures, neurologic outcome (NIHSS) @ 1 year
D: prospective randomized, double-blind, placebo-controlled clinical trial
N =72, VPA =36, Pbo =36
癲癇總發生率21%,兩組間發生率無顯著差異,但VPA可減少早期癲癇。
VPA可以改善NIHSS分數。
缺點:病例數太少。
#2. Prospective, randomized, single-blinded comparative trial of intravenous levetiracetam versus phenytoin for seizure prophylaxis. Neurocrit Care. 2010 Apr;12(2):165-72. PMID: 19898966.
P: severe traumatic brain injury (sTBI) or subarachnoid hemorrhage 外傷性腦出血
I/C: iv levetiracetam (LEV) vs. iv phenytoin (PHT) 2:1 ratios
O: seizure occurrence (diagnosed by cEEG), Disability Rating Scale score @ 3 months, Glasgow Outcomes Scale score @ 6 months, mortality, side effects
D: prospective, single-center, randomized, single-blinded comparative trial
N =52 (89% sTBI), LEV =34, PHT =18
LEV vs PHT
早期癲癇: 14.7% vs 16.7% 無顯著差異
6個月癲癇: 5% vs 0% 無顯著差異 (咦...)
長期預後較好 (DRS score, GOS score)
死亡率: 41% vs 22% 無顯著差異 (哇......)
腸胃副作用較高。
缺點:病例數更少,和我的病人不符,死亡率有偏高傾向!
#3. Prophylactic antiepileptic drug use is associated with poor outcome following ICH. Neurocrit Care. 2009;11(1):38-44. PMID: 19319701.
P: patients within 6 h of the onset of acute ICH (placebo arm of Cerebral Hemorrhage and NXY-059 Trial)
I/C: early prophylactic antiepileptic drugs (AEDs)
O: poor modified Rankin Scale of 5 or 6 (severely disabled or dead) @ 90 day
D: international multicenter randomized trial >> clinical trial cohort
N =295, 腦出血量中位數14.9 (IQR 7.9-32.7); 平均數23.3 (SD 22.8) ml
癲癇發生率1.7%,第90天嚴重預後(mRS 5 or 6) 28%
早期預防抗癲癇藥物使用於8%的病人,這群病人嚴重預後風險較高 (OR 6.8; 95% CI: 2.2-21.2)
缺點:非隨機對照,僅為控制組世代的病例對照研究,易有選擇性偏差。
那到底要不要使用預防性抗癲癇藥物?
1. 發生癲癇就需治療。
2. 專家建議 (神外),畢竟病患是他們照顧。
3. 證據說話:要看病患族群(自發性vs外傷性出血),癲癇發生率(地區流病調查),選用藥物來看。
第一篇癲癇預防無啥效,但長期預後好。第二篇是外傷病患,不符所需。第三篇使用藥物反而預後差。
眾說紛紜何時了? 大家看著辦吧!
...
沒有留言:
張貼留言